Improving Patient SDoH Through Community Health Workers
Clinic details
FQHC look-alike
Staff includes:
3 Physicians
1 APRN
2 PA
2 NP
1 LMSW
2 MAs
1 Quality Coordinator
1 Dietician (part-time)
Project Description
Goal: Improve health outcomes for high-risk patients with SDoH-related needs through a standardized process for identification and referral to a community-based Community Health Worker (CHW).
Methods:
1) Identify patients with chronic conditions and SDoH needs through a standardized screening.
2) Refer patients with 2+ chronic conditions and 1 SDoH need to a community-based CHW.
2) Develop a reimbursement strategy for financial sustainability.
Results
From January to June 2025:
1,089 patients were screened using the PRAPARE tool (overall positivity rate unknown)
From June 1 to August 18, 2025:
476 patients were screened using the PRAPARE tool. Positive screening results showed:
Food Insecurity: 28/347 (8%; No Answer=119)
Housing Insecurity: 16/450 (3.6%; No Answer=25)
Financial Insecurity: 49/366 (13%; No Answer=109)
Transportation Insecurity: 22/398 (5.5%; No Answer=117)
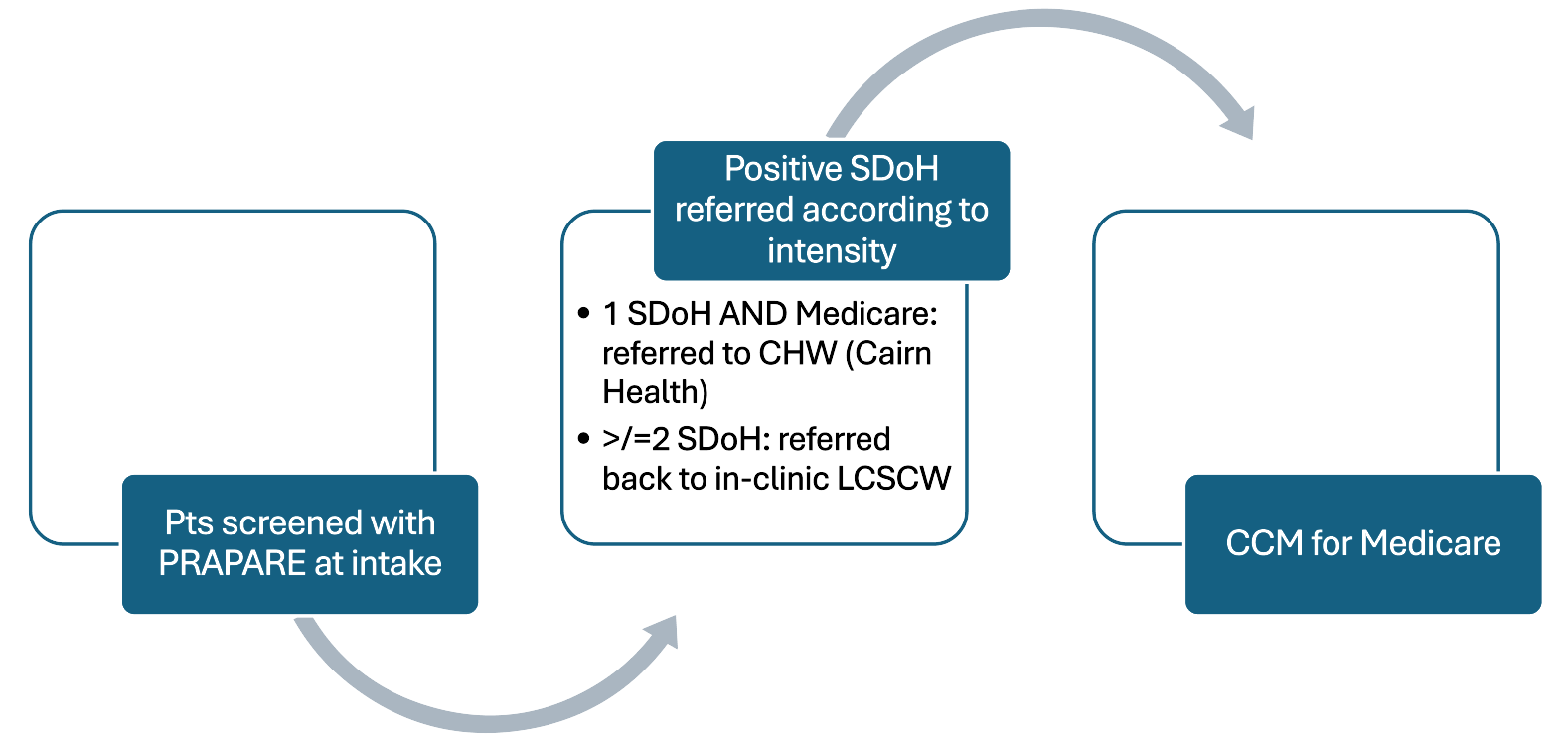
Baseline workflow: